Chapter 53 – Dawn Murtagh (D3SOP13)
Domain 3 Standard of Proficiency 13
Be able to comply with relevant and current health and safety legislation and guidelines and be able to access recommendations and findings of inquiries, investigations and associated reports relevant to social care.
|
KEY TERMS Compliance Health and safety legislation Inquiry reports Accessing reports and recommendations
|
Social care is … about providing the best quality of care possible, treating the people we work with as we would like our own family members to be treated. Social care involves promoting independence, encouraging people to reach their full potential and achieve their goals. Advocating for people while also providing them with the skills to advocate for themselves. Focusing on the positives even in times when this may seem difficult. Providing a person-centred approach, recognising that every person is different with their own individual needs and strengths. |
Introduction
This standard of proficiency has two main elements. First, it requires social care workers to comply with relevant and current health and safety legislation and guidelines. Second, social care workers must be able to access the recommendations and findings of inquiries, investigations and associated reports relevant to social care. Utilising my research and experience with young people in residential and disability services, this chapter will explore what it means to comply with current health and safety legislation and guidelines in social care, explained through practical tips and links on how to access findings and recommendations of relevant reports.
Compliance
What it means to comply
Compliance is the process of adapting, following or acting in accordance with rules and guidelines that relate to best practice (Dunbar 2021). It can be understood as behaviours fitting to how one should or should not act in accordance with regulations, standards or legislation (Dunbar 2021; Etienne 2012). In order for there to be a willingness to comply, it must be understood why compliance is important. Compliance with regulations, policies and legislation is vital for safe practice, to enable the smooth running of an organisation and to guarantee that everyone understands what is expected of them, as well as ensuring that everyone follows correct procedures.
Complying with standards in social care helps organisations to improve and maintain a high quality of care. For example, when preparing meals in a residential setting, compliance with food safety regulations ensures that food is handled, stored and prepared correctly, preventing cross-contamination and food poisoning. Complying with hygiene regulations prevents the spread of illness or infection.
TASK 1
Check out the Health and Safety Authority website (http://hsa.ie) and find out their role in health and safety in the workplace.
Everything we do in social care encompasses health and safety legislation and guidelines. These play a vital role in the provision of social care, protecting the safety and wellbeing of service users, staff, volunteers and anyone involved in a service. Health and safety regulations help identify potential hazards, therefore reducing and preventing the occurrence of accidents, injury or fatality. But first what is the difference between legislation and guidelines? Legislation is an Act or law that has been set out by government. It is legally binding and therefore must be adhered to (Furlong 2014; Kenneally & Tully 2013). Guidelines interpret legislation and advise how to comply with the legislation, but they are not enforced by law.
TASK 2
Read Chapter 9 to learn about the role of policies and systems in protecting the health, safety and welfare of staff, service users and volunteers.
Health and Safety Legislation
One of the main pieces of legislation governing occupational health in Ireland is the Safety, Health and Welfare at Work Act 2005. This legislation applies to all places of work and has a major influence on our day-to-day practice in social care. Its purpose is to guarantee the health, safety and welfare of people at work. It places a duty of care on employers to manage work activities as much as reasonably practicable to prevent injury and ill-health and ensure the safety and welfare of employees. Under the Act employees are required to take reasonable care for their own safety and the health and safety of anyone impacted by their work.
TASK 3
Have a look around your home and see if you can identify any potential hazards that could cause harm. Who could they harm and how? How likely is this to happen? How serious could it be? What could be put in place to prevent or reduce the risk of harm?
Risk Assessments
TASK 4
Read Chapter 52 by Grace O’Flynn to learn more about risk analysis and risk management.
Section 19 of the Safety, Health and Welfare at Work Act 2005 requires that all organisations must conduct risk assessments which must be reviewed on a regular basis and amended where necessary. It is the duty of all social care workers to conduct risk assessments.
|
STEPS INVOLVED IN CONDUCTING RISK ASSESSMENTS |
|
(i) Identify hazards. A hazard can be construed as anything that can cause harm. These include physical hazards, such as manual handling, using vehicles, slips and falls, chemical hazards (e.g. cleaning products), biological hazards (e.g. infection or allergies) and psychological hazards such as bullying or aggressive behaviour. |
|
(ii) Assess the risk. This entails deciding who is at risk of harm due to the identified hazards. It also must be considered how probable it is for harm to occur and the extent of the impact of that harm. |
|
(iii) Put measures in place to eliminate or prevent harm from occurring as much as reasonably practicable (HSA 2012; Safety, Health and Welfare at Work Act 2005). |
Case Study 1
Mary has recently been referred to a residential care facility. During her initial assessment Mary’s parents notified staff that Mary has an allergy to nuts. Before Mary attends the facility, a risk assessment was carried out and safety procedures put in place. The hazard identified in this case is nuts and any food products containing nuts. Assessing the risk identified that the person at risk from this hazard is Mary. No other staff or service users are deemed at risk because none of them has a nut allergy. Due to Mary’s allergy, it is highly probable that she will experience harm or adverse reaction if she comes into contact with nuts. The extent of the impact is high: Mary could experience a severe allergic reaction, anaphylactic shock leading to fatality, depending on the severity of her allergy. Measures that could be put in place to prevent/reduce harm include enforcing a ‘no nuts’ policy in the residential centre. Other residents and families must be told not to bring nut products into the centre. Nuts must not be used in the preparation of meals and labels must be checked when shopping. Staff are trained in the use of an EpiPen in the case of anaphylaxis. An emergency protocol must be put in place to follow in the event of an adverse reaction.
Safety Statements
Section 20 of the Safety, Health and Welfare at Work Act 2005 requires every organisation and employer to have a written safety statement specifying all identified hazards and risks which have been assessed. The safety statement must outline staff duties and measures taken to protect their health, safety and welfare at the place of work. Additionally, it must include emergency and evacuation procedures.
TASK 5
When on placement read your organisation’s safety statement. It is important to be aware of any emergency procedures and the duties involved to ensure safety.
Additionally, the Act sets out fines and penalties for breaches of health and safety legislation. The Safety, Health and Welfare at Work (General Application) Regulations 2007 provide more extensive detail on specific topics, for instance pregnancy at work, manual handling, the physical environment such as electricity and signage, workplace and personal protective equipment, first aid, training, night work and shift work and the protection of children, etc.
Slips, trips and falls are very common causes of injury in the workplace. Organisations are required to maintain a safe environment to prevent slip or trip hazards (HSA 2012). This is particularly important when working with people with visual impairments, mobility issues or physical disabilities. Floor space and exits must be kept clear at all times. Where I work, doors are painted a highly contrasted colour to walls to make them clearly visible. Steps and stairs are fitted with hand rails and high-visibility strips. A cleaning protocol is in place for staff to follow. Floors must be cleaned when there is little to no traffic. Spills must be cleaned immediately. Bright and even lighting is installed throughout the house. A policy is in place for reporting accidents.
There can be some drawbacks to health and safety guidelines. For instance, the requirement for emergency exit lights and safety signs in disability and residential care facilities can create a cold, clinical look in a place that is supposed to be inviting and homely for young people. This has become more evident during the COVID-19 pandemic as services have been required to display social distancing graphics and COVID-19 information posters.
The nature of service provided and the needs of the people we work with must be taken into consideration when implementing health and safety regulations as, on occasion, the implementation of a safety requirement can create risk in itself. For example, in relation to fire safety, it is a requirement under the Health Act 2007 (as amended) for residential houses to have automatic closing fire doors (HIQA 2021). While these are vital in the event of a fire for preventing its spread and allowing time for evacuation, they can be hazardous. These doors are expected to be kept closed when not in use. Fire doors are very heavy, which creates an obstacle for people with physical disabilities. Measures need to be put in place to eliminate impediments or dangers. For instance, a hold-open device can be installed to ensure that the fire door does not create a barrier for people with disabilities or mobility issues. When a fire alarm goes off these doors will close automatically.
This poses a difficulty for the students with visual impairments I work with, as they are unable to see that the doors are closing. To ensure students don’t collide with the doors, they are reminded during regular fire drills to take care when approaching the doors as they will be swinging closed. Personal emergency evacuation plans are in place that take into consideration the needs of each individual when evacuating a building.
National Standards
Both the National Standards for Children’s Residential Centres (2018) and the National Standards for Residential Services for Children and Adults with Disabilities (2013) set out by the Health Information and Quality Authority (HIQA) emphasise the provision of safe care, and protecting people from harm, neglect or abuse. The standards mandate that all incidents that occur are managed and scrutinised to inform practice and prevent future harm. Additionally, the standards require the promotion of wellbeing and ensure that people’s individual health needs are met. The Children First Act 2015 was aimed to make better provision for the protection of children. Under the Act, all children’s services are required to have a safeguarding statement. The act enforces the obligation of mandated persons to report any concerns to Tusla, the Child and Family Agency. Furthermore, the Act provided the legal basis for Children First: National Guidance for the Protection and Welfare of Children (2017). This document establishes clear guidelines for recognising and reporting abuse and neglect. It describes the four main types of abuse and how to identify them. It highlights the steps involved in reporting concerns. The role and responsibilities of a mandated person are established, along with protocols for social workers working in Tusla.
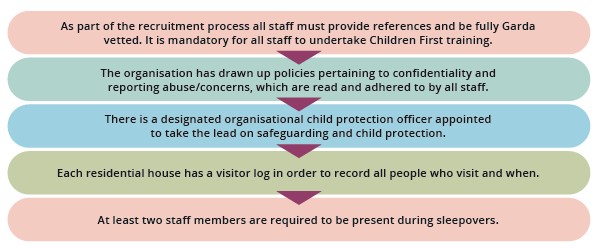
To promote safety and protect young people (3.1 of National Standards for Residential Services for Children with Disabilities) and comply with the Children First Act, the organisation I work with put the following protocols in place.

Case Study 2
The following case study is an example of how an organisation practises in line with national standards. This is a fictional scenario, not based on real events.
4.1 promoting the health and development of each child:
Jack is a 14-year-old boy who has recently started living in a residential house for students with visual impairments. He lives in the house from Sunday to Friday, attends school and goes home at the weekends. At home, he lives with his parents and older brother. Jack has recently lost the majority of his vision. Before attending the service, Jack’s needs were assessed in order to put an individualised plan in place to address these needs, establish goals to work towards and provide meaningful care and support. The service provided Jack with an ophthalmology exam to assess his vision and eye health. A personal medical care plan will be written to address Jack’s medical needs. Access to nurses, dental screening, occupational therapy or physiotherapy will be available to if desired. Jack takes medication for high blood pressure. All staff have received medication training. Two staff must be present and medication administration protocol must be followed when giving Jack his medication. Jack will be supported to self-administer his medication. Medication audits are carried out on a regular basis to guarantee that proper procedure is being followed. If a medication error occurs this must be reported immediately, the nursing team must be informed to provide medical advice and an error form is to be filled out. As Jack has recently lost vision, he is receiving orientation and mobility training to gain the skills necessary to navigate his surroundings without accident or injury. Jack has expressed an interest in learning how to access local shops and parks and travelling to school independently. These objectives will be added to his care plan and an orientation and mobility specialist will work with Jack to achieve his goals.
Jack will learn new independent living skills in order to adapt to his vision loss. For example, a programme will be put in place to safely teach Jack how to pour liquids or make hot drinks safely. Adaptions are made to appliances, such as tactile stickers, so that Jack can use them independently without sight.
Staff are building positive relationships with Jack. He is provided with the opportunity to express his opinions and make his own choices regarding all aspects of his care. He has a say in what activities he would like to partake in, meal choices, etc. This can be achieved on a daily basis and through link sessions with his key/link worker. Jack’s grandmother, to whom he was very close, has recently passed away. During link sessions, Jack is provided with a safe space to express his emotions. He is reassured that all staff are there to support and listen to him whenever he needs. Jack’s link worker offered to source counselling for Jack if he wishes.
It has been observed that Jack’s favourite foods are Chinese takeaway and burgers and chips. He eats very little fruit or vegetables and drinks a lot of fizzy drinks. Jack seems to have very little awareness about nutrition and healthy eating. After discussion Jack has agreed to partake in an education programme to learn about healthy eating, nutrition and exercise. Jack expressed an interest in learning how to prepare his own snacks and lunch for school. Staff will teach Jack kitchen safety. He will be supervised and given the skills necessary to use sharp knives, handle hot objects and use appliances such as microwave, oven or toaster.
Inquiries, Reports and Recommendations
As we know, a plethora of inquiries and reports have had a major influence in shaping the landscape of social care practice in Ireland. These reports include the Kennedy Report (1970), the Madonna House Report (1996), the Newtown House Report (2001), the Ryan Report (2009) and the Child in Care Death Report (2012). The recommendations of these reports, along with others, have brought about significant change leading to improvements in the provision of care for the people we work with. Inquiries help establish what happened in the past and learn from mistakes (LRC 2005).
However, many have criticised the effectiveness of reports (Burgess 2009, 2011; Mackie 2012; Stutz 2005). Burgess (2009) has claimed that inquiry reports have been ineffective, overly time-consuming, expensive and ineffective. He also argued that these reports placed too much focus on laying blame and introduced too many regulations without considering possible consequences. Howard (2012) has debated that while regulation and maintaining records is vital for transparency and accountability, over-regulation and excessive recording of information can often take the humanity out of care.
Professionals often work in fear of allegations being made against them and have to balance the conflict between meeting the demands of paperwork and caring for the people they work with. Young people are acutely aware of the level of recording conducted. ‘Are you going to write that in my daily log?’ and ‘What are you going to write about me?’ are questions I have regularly been asked by young people I work with. We must consider how this makes them feel. The Ombudsman for Children (Muldoon 2017) says, ‘It is important that Tusla operates in a way that protects the child rather than the system.’ From their research, Buckley and O’Nolan (2013) advised that future inquiries should limit their recommendations and place emphasis on key learning points which could be integrated into future practice across all organisations.
HIQA, which was established under the 2007 Health Act, is an independent authority whose purpose is to set standards to promote a safe, high quality of care by health and social care services. It monitors and inspects services to ensure these standards are being met and that services provide safe, effective care that meets the needs of service users (Health Act 2007). When carrying out inspections HIQA determines a service’s level of compliance, or non-compliance, with the national standards.
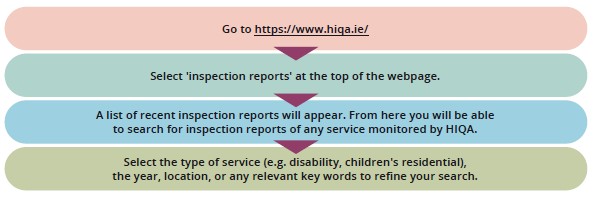
Accessing HIQA inspection Reports
TASK 6
Practise this by looking up inspection reports for the service where you are on placement.
![]() Tips for Practice Educators
Tips for Practice Educators
- Inform students of legislative material and guidelines regarding health and safety relevant to social care.
- Discuss the role of inspections and provide information on some of the main inquiry reports that have had a major influence on the landscape of social care.
- Allow students the opportunity to practise accessing inspections and reports.
References
Buckley, H., and O’Nolan, C. (2013) An examination of recommendations from inquiries into events in families and their interactions with state services, and their impact on policy and procedure. Dublin: Government Publications.
Burgess, A. (2011) ‘The changing character of public inquiries in the (risk) regulatory state’, British Politics, 6(1): 3-29.
Burgess, A. (2009) Public Inquiries and the Management of Public Risk, Report commissioned by the Risk and Regulation Advisory Council. London: Risk and Regulation Advisory Council.
Children First Act (2015) Dublin: Stationery Office.
Department of Health (1996) Report on the Inquiry into the Operation of Madonna House. Dublin: Stationery Office.
Dunbar, P., Browne, J.P. and O’Connor, L., (2021) Determinants of regulatory compliance in health and social care services: a systematic review protocol. HRB Open Research, 4(13) Available at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8258703.3/
Etienne, J., (2011) Compliance theory: A goal framing approach. Law & Policy, 33(3): 305-333.
Furlong, J., (2014) Free and Easy: A Guide for Occasional Users for the Irish Legal System and Resources Legal Information Management. 14: 276-282.
Health Act, (2007) Dublin: Stationery Office.
Health Information and Quality Authority, (2018) The National Standards for Children’s Residential Centres. Dublin: Stationery Office.
Health Information and Quality Authority, (2013) The National Standards for Residential Services for Children and Adults with Disabilities. Dublin: Stationery Office.
Health and Safety Authority, (2012) Health and Safety at Work in Residential Care Facilities. Available at https://www.hsa.ie/eng/Publications_and_Forms/Publications/Healthcare_Sector/Health_and_Safety_at_ Work_In_Residential_Care_Facilities1.html.
HIQA (Health Information and Quality Authority) (2021) Fire Safety Handbook: A Guide for Providers and Staff of Designated Centres. Dublin. Available at <https://www.hiqa.ie/sites/default/files/2021-02/Fire- Safety-Handbook-a-guide-for-providers-and-staff-of-designated-centres.pdf> [accessed 10 August 2021].
Kenneally, A. and Tully, J. (2013) The Irish Legal System. Ireland: Clarus Press.
Kennedy, E. (1970) Reformatory and Industrial Schools System Report. Dublin: Stationery Office.
Law Reform Commission (2005) Report on Public Inquiries including Tribunals of Inquiry. Dublin: Law Reform Commission.
Mackie, K. (2012) Public Inquiries – Proposals for a Design Rethink. Inquiry into Public Inquiries Consultation Draft 2 December 2012. London: Centre for Effective Dispute Resolution
OECD (organisation for Economic Co-operation and Development’ (2002) Reducing the Risk of Policy Failure: Challenges for Regulatory Compliance. Available at https://www.oecd.org/regreform/regulatory- policy/1910833.pdf
Office of the Minister for Children and Youth Affairs. (2009) Report of the Commission to Inquire into Child Abuse, 2009 Implementation Plan. Dublin: Stationery Office.
Safety, Health and Welfare at Work Act (2005) Dublin: Stationery Office.
Safety, Health and Welfare at Work (General Application) Regulations (2007) Dublin: Stationery Office.
Shannon, G. and Gibbons, N. (2012) Report of the Independent Child Death Review Group. Dublin: Government Publications.
Social Services Inspectorate (2001) Newtown House High Support Unit Inspection Report. Dublin: Stationery Office.
Stutz, J.R. (2005) ‘What gets done and why: Implementing the recommendations of public inquiries’. Canadian Public Administration, 51(3): 501-21.
